

Knee osteoarthritis is one of the most common reasons people walk into our sports chiropractic office in Murray, and it is also one of the most misunderstood. In Part 1, we described knee osteoarthritis (OA) as a whole-joint condition driven by a mismatch between joint load and its capacity to handle it. That framing is useful because it points directly to what you can influence. This article covers the factors that raise your risk, the strategies that genuinely help with prevention, what the nutrition research does and doesn’t support, and the signs that mean it’s time to have your knee looked at.
What Raises Your Risk of Knee Osteoarthritis?
Some risk factors are outside your control. Age increases risk; women are affected more often than men; genetics play a role; and a previous significant knee injury, such as an ACL tear, meniscus damage, or fracture, raises the odds of developing OA in that joint years later. Joint alignment and anatomy matter too.
The good news is that several of the most powerful risk factors are modifiable. Body weight is at the top of that list. Excess weight increases the mechanical load through the knee with every step, but it also contributes through metabolic and inflammatory pathways, which is why obesity is linked to OA even in non-weight-bearing joints. Research consistently shows that higher body weight is associated with both a greater risk of developing knee OA and more severe pain and functional limitation once it is present. 1 6 Other modifiable contributors include weak or deconditioned muscles around the knee and hip, occupations or activities involving heavy repetitive loading, and poorly managed prior injuries.
A Quick Anatomy Review
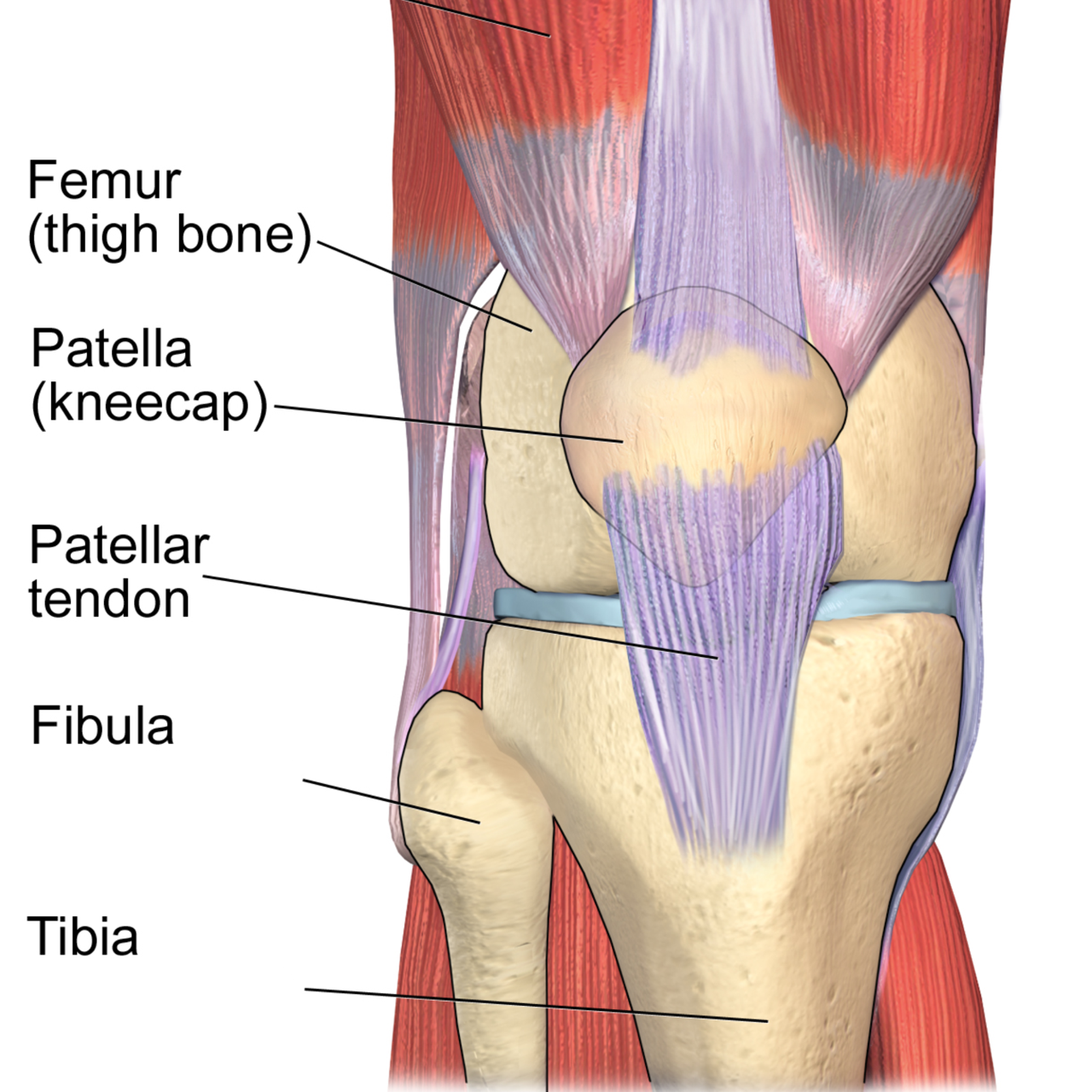
Between the femur and tibia sit two C-shaped shock absorbers called the menisci. They spread the load across the joint, add stability, and protect the cartilage underneath. Surrounding the whole joint is a capsule lined with synovium, a thin membrane that produces synovial fluid to lubricate and nourish the cartilage. Ligaments such as the ACL, PCL, LCL, and MCL hold the bones in alignment, while the muscles that cross the knee, especially the quadriceps and hamstrings, control movement and absorb force. Just beneath the cartilage lies the subchondral bone, which plays a bigger role in osteoarthritis than most people realize.
What Actually Helps to Prevent Osteoarthritis (or slows it down)
Because weight is such a strong and modifiable driver, weight management is one of the highest-yield prevention strategies available. A meta-analysis of observational studies estimated that preventing obesity could meaningfully reduce the incidence of knee osteoarthritis at the population level by almost 30. 2 For someone already carrying extra weight, even modest weight loss reduces knee load and symptoms.
Staying active is the second pillar. Contrary to the old fear that exercise “wears out” the knees, regular moderate activity and strong supporting muscles protect the joint by improving its capacity to absorb load. Keeping the quadriceps, hamstrings, and hip muscles strong, maintaining good range of motion, and addressing prior injuries properly all help keep the load-to-capacity balance in your favor. We will cover the specifics of exercise in Part 4 of this series.
How Can Your Nutrition Affect Your Risk of Osteoarthritis?
Patients often ask which foods or supplements will fix their knees. It’s worth being honest here: no diet or supplement reverses established osteoarthritis, and the marketing around joint supplements far outpaces the evidence. That said, nutrition is not irrelevant. 3
The strongest dietary evidence supports an overall healthy, anti-inflammatory eating pattern. Something similar to a Mediterranean-style diet rich in vegetables, fruit, whole grains, fish, and healthy fats, and lower in ultra-processed foods and added sugar. Long-chain omega-3 fatty acids (from oily fish) and adequate vitamin D are frequently discussed, and correcting a genuine deficiency is reasonable, but evidence that isolated supplementation alters the disease course is limited. 3 4 Popular products like glucosamine and chondroitin have mixed reviews, with some patients having good relief with consistent use, but major studies and guidelines do not strongly recommend them. 5
The practical takeaway: use nutrition to manage weight and support overall health rather than chasing a single “joint miracle” supplement. If you’re considering supplements, it’s worth discussing them with your healthcare team to find the best options for your particular concerns.
When Should You Seek Care for Your Knee Pain?
Knee pain is easy to dismiss, but certain signs mean you shouldn’t wait. Consider getting your knee evaluated if you have pain that persists for more than a few weeks, pain that limits walking, climbing stairs, work, or sleep, ongoing swelling, a knee that locks, catches, or gives way, or stiffness that consistently lingers after rest.
NOTE: Rapidly worsening pain, a hot and visibly swollen joint, fever, or an inability to bear weight warrants prompt medical attention, as those can signal something other than routine osteoarthritis.
Seeking care early has a real advantage: the sooner you address strength, movement, and load, the more you can do to keep the joint functioning well and avoid the deconditioning spiral described in Part 1. Guidelines recommend starting with conservative, active management rather than jumping to imaging or surgery for most people. 5
In Part 3, we’ll walk through exactly how we care for knee osteoarthritis at Revive Sport & Spine, including soft-tissue therapy, joint manipulation, and shockwave therapy, and how these approaches set the stage for the rehab exercise plan in Part 4.
Key Takeaways Before We Progress to Part 3
✓ Excess body weight through diet and exercise is one of the strongest and most modifiable risk factors for knee osteoarthritis. 1 2
✓ No supplement “cures” OA, but weight management and an overall healthy, anti-inflammatory dietary pattern have the best evidence. 3 4
✓ Persistent swelling, locking, giving way, or pain that limits daily life are signals to get your knee evaluated. 5
If your knee has been nagging or you have risk factors and want to stay ahead of osteoarthritic changes and pain, an assessment is a smart first step. We’ll assess your movement, strength, and daily load and help you develop a realistic prevention or management plan.
Frequently Asked Questions
What is the biggest risk factor for knee osteoarthritis?
Excess body weight is among the strongest and most modifiable risk factors. It increases mechanical load on the knee, drives inflammation, and is linked to both developing OA and worse symptoms. 1 2 6
Can knee osteoarthritis be prevented?
You can’t change age or genetics, but you can lower your risk by maintaining a healthy weight, staying active, keeping the muscles around the knee strong, and properly rehabilitating any knee injuries. Preventing obesity alone could reduce up to 30% of knee OA cases. 2
What is the best diet for knee osteoarthritis?
There is no magic food, but the best-supported approach is using nutrition to reach and maintain a healthy weight alongside an overall anti-inflammatory, Mediterranean-style pattern rich in vegetables, fish, and healthy fats. 3 4
Do glucosamine and chondroitin work for knee arthritis?
While some patients swear by it, high-quality trials show inconsistent results, and major clinical guidelines do not strongly recommend them. They are generally safe, but they should not replace weight management, exercise, a reasonable diet, and appropriate care. 5
When should I see someone about knee pain?
Get evaluated if pain lasts more than a few weeks, limits daily activities, or is accompanied by swelling, locking, or giving way. A hot, swollen joint with fever or an inability to bear weight needs prompt emergency medical attention. 5
REFRENCES
1. Batushansky A, et al. Obesity-Related Knee Osteoarthritis — Current Concepts. (Review). 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10456094/
2. Zheng H, Chen C. What if we prevent obesity? Risk reduction in knee osteoarthritis estimated through a meta-analysis of observational studies. Arthritis Care & Research. 2011. https://pubmed.ncbi.nlm.nih.gov/21425246/
3. Diet in Knee Osteoarthritis — Myths and Facts. Nutrients. 2025;17(11):1872. https://www.mdpi.com/2072-6643/17/11/1872
4. Thomas S, et al. What is the evidence for a role for diet and nutrition in osteoarthritis? Rheumatology. 2018;57(suppl_4):iv61-iv74. https://academic.oup.com/rheumatology/article/57/suppl_4/iv61/4975692
5. Bannuru RR, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis and Cartilage. 2019;27(11):1578-1589. https://pubmed.ncbi.nlm.nih.gov/31278997/
6. Onishi K, et al. Level of obesity is directly associated with the clinical and functional consequences of knee osteoarthritis. Scientific Reports. 2020;10:3601. https://www.nature.com/articles/s41598-020-60587-1